Case
Case
- Index
- Case1:
Restenosis at the bifurcation treated by crush stenting,
60 year old male - Case2:
A long lesion in right coronary artery,
70 year old female - Case3:
Shepherd Crook Type RCA,
60 year old male - Case4:
Retrograde approach for chronic total occlusion in RCA,
70 year old female - Case5:
High take-off vein graft,
60 year old male - Case6:
Anomalous origin of RCA from left coronary sinus,
50 year old male - Case7:
A case of RCA CTO
by Dr. Chiung-Jen Wu and Dr. Swapnil Mate
Case4: Retrograde approach for chronic total occlusion in RCA, 70 year old female
Case
The patient with triple vessel disease underwent coronary artery bypass surgery 9 years ago. RCA was total occlusion. Bypass grafts were LITA-LAD, SV-Cx and SV-RCA. She has been free from angina for 9 years. However, angina recurred.
Coronary angiography showed a total occlusion of SV-RCA. Native RCA was also total occlusion with collateral flow from Circumflex.
Coronary angiography
Chronic total occlusion of RCA with calcification more than 9 years old, Collateral flow from circumflex.
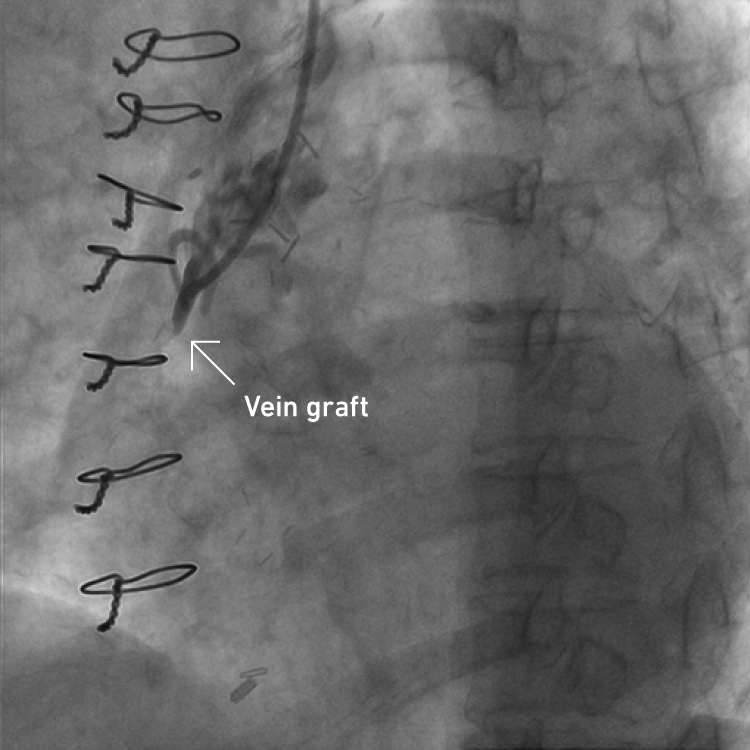
Total occlusion of SV-RCA
RCA 6F IL3.5 TFI, LCA 6F IL3.0 TRI
An antegrade guidewire failed to pass into a true lumen confirmed by the retrograde angiography.
Retrograde approach
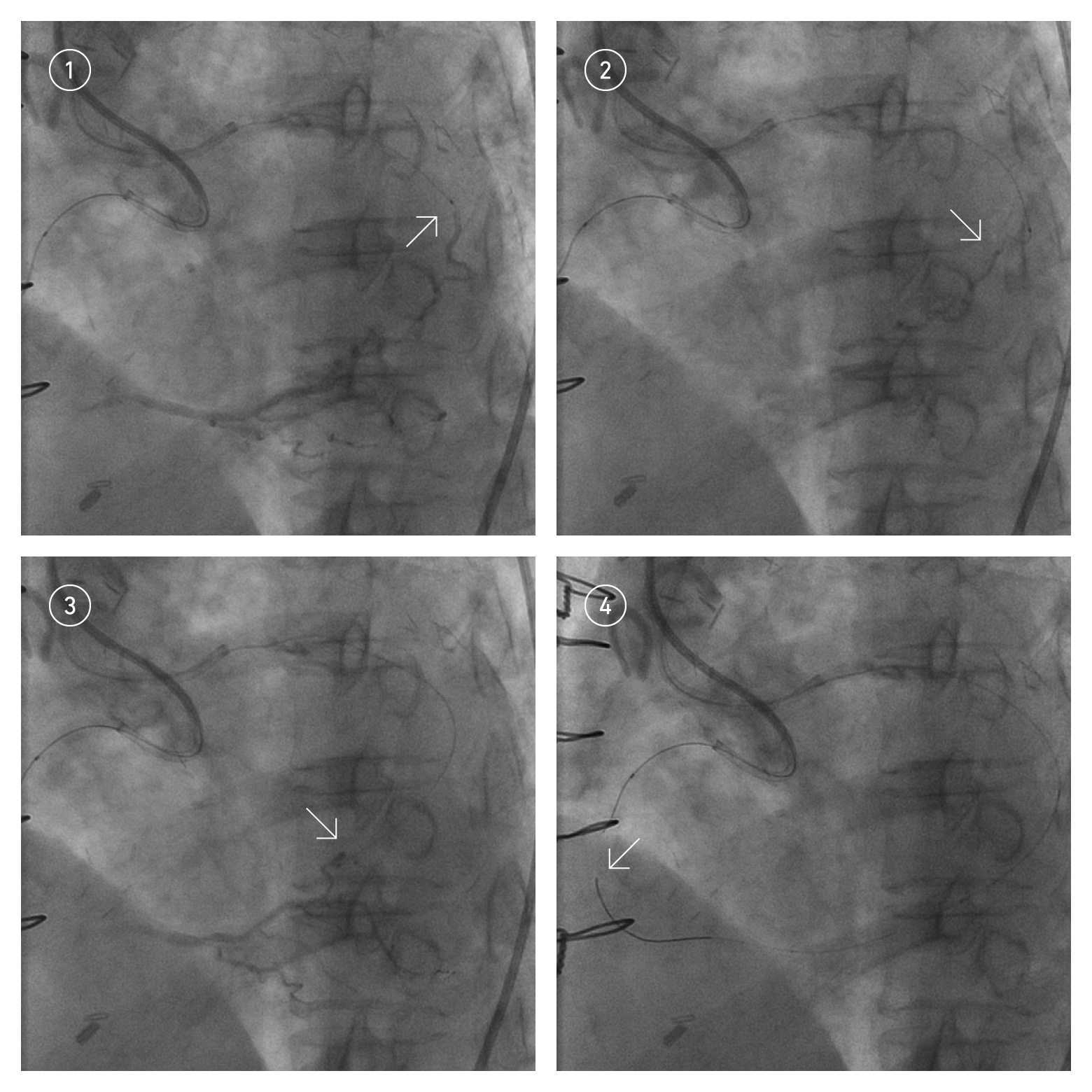
From circumflex, a Fielder FC wire with finecross MG 150cm were passed. The arrow indicates the distal tip of the retrograde guidewire.
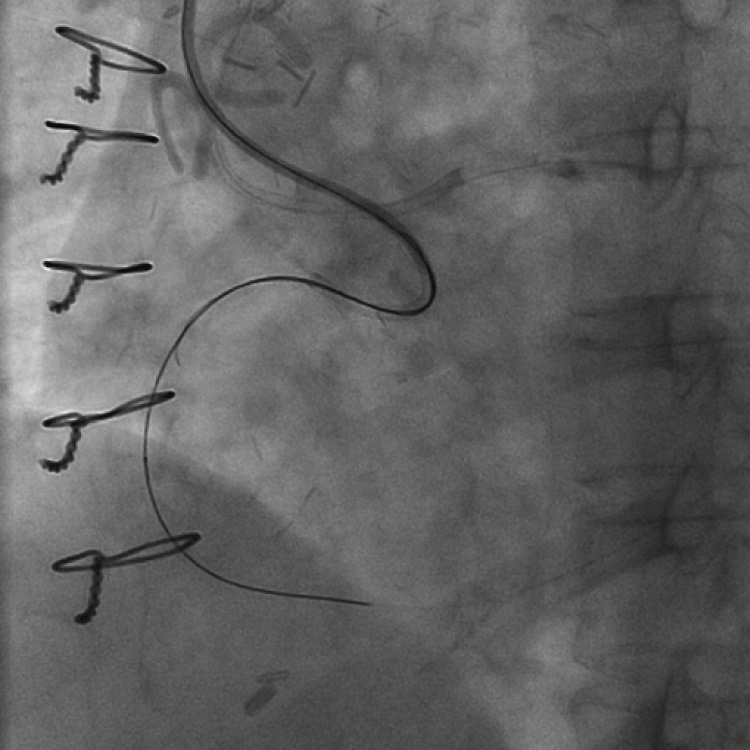
The retrograde guidewire passed the CTO lesion and was inserted into the antegrade guiding catheter. A microcatheter was also inserted into the antegrade guiding catheter and then the guidewire was changed to a 3m long guidewire. The long guidewire was inserted into the retrograde guiding catheter and extracted from the antegrade guiding catheter.
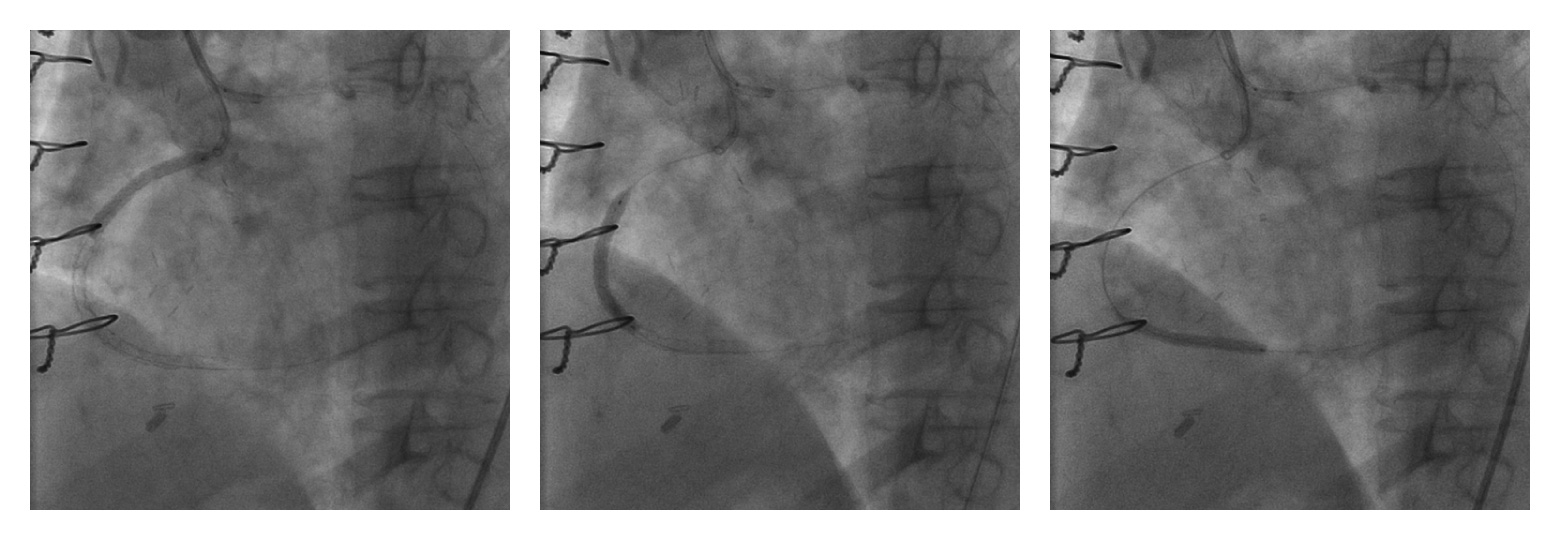
Three stents were implanted.
Final angiography
Summary
CTO lesions more than 9 years old were successfully treated by retrograde approach. Two 6F Ikari L guiding catheters were used for left and right coronary arteries.
Power position of Ikari L can generate great backup force. It is possible to perform CTO PCI using 6Fr Ikari L.
