Case
Case
- Index
- Case1:
Restenosis at the bifurcation treated by crush stenting,
60 year old male - Case2:
A long lesion in right coronary artery,
70 year old female - Case3:
Shepherd Crook Type RCA,
60 year old male - Case4:
Retrograde approach for chronic total occlusion in RCA,
70 year old female - Case5:
High take-off vein graft,
60 year old male - Case6:
Anomalous origin of RCA from left coronary sinus,
50 year old male - Case7:
A case of RCA CTO
by Dr. Chiung-Jen Wu and Dr. Swapnil Mate
Case6: Anomalous origin of RCA from left coronary sinus, 50 year old male
Case
Maintenance hemodialysis was started due to diabetic nephropathy 5 years ago.
He felt chest pain on effort 5 months ago. Three weeks ago, chest pain happened during hemodialysis.
Coronary angiography showed CTO in RCA. But the RCA was originated from left coronary cusp anomalously.
PCI failed in another hospital.
RCA was originated from left coronary cusp
Extremely severe calcification due to renal failure.
Anomalous origin
Because radial artery was used for shunt to perform hemodialysis, we selected femoral access in this case.
7 Fr Ikari L 4
Power position
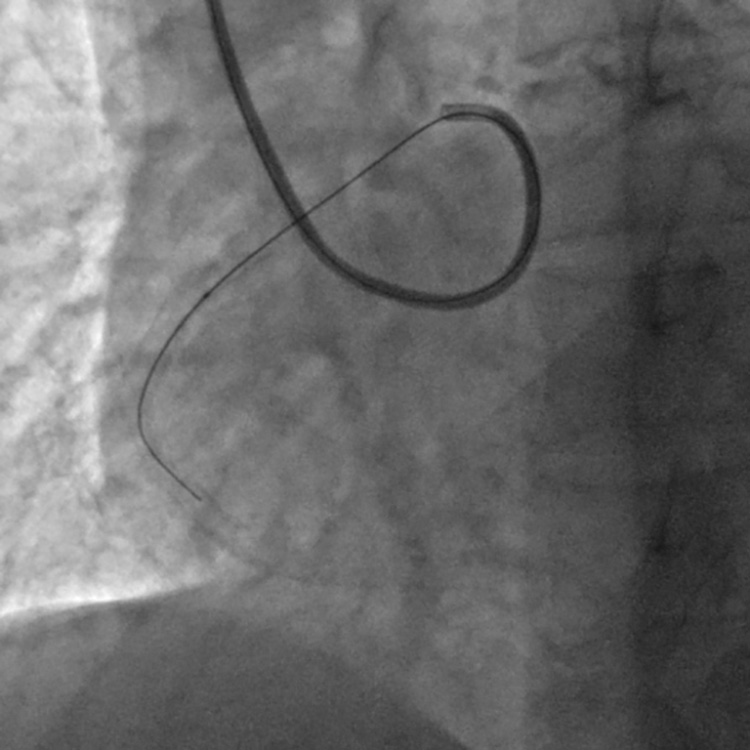
It is sometimes difficult to engage a guiding catheter for this anomaly. However, Ikari L is easy to engage. Also, power position is easily made by pushing the guiding catheter. It increased backup force.
The conquest (confienza) guidewire passed the lesion successfully with power position of Ikari L.
Due to extremely severe calcification, it was necessary to use guiding catheter extension with power position to pass the CTO lesion.
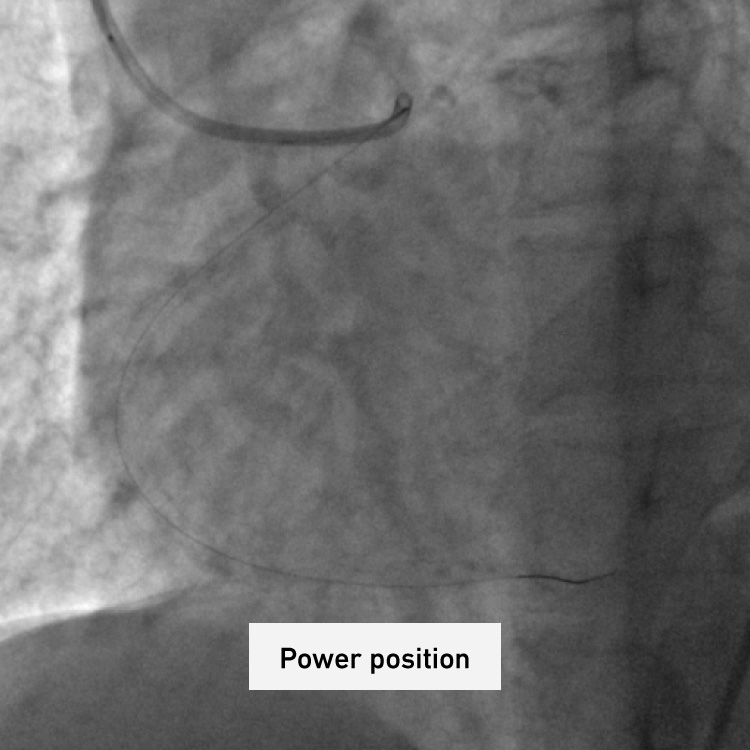
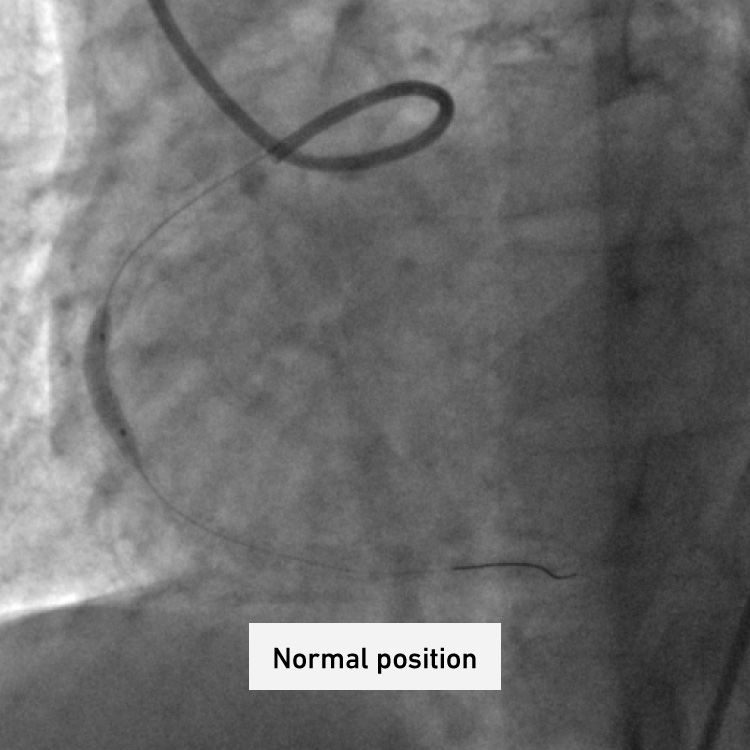
It is easy to make power position and it is also easy to come back to normal position.
Final angiography
Summary
A RCA CTO lesion with anomalous origin from left coronary sinus was successfully treated using Ikari L even though it failed in another hospital.
Ikari L is easy to engage and easy to make power position for this type of anomaly.
