Case
Case
- Index
- Case1:
Restenosis at the bifurcation treated by crush stenting,
60 year old male - Case2:
A long lesion in right coronary artery,
70 year old female - Case3:
Shepherd Crook Type RCA,
60 year old male - Case4:
Retrograde approach for chronic total occlusion in RCA,
70 year old female - Case5:
High take-off vein graft,
60 year old male - Case6:
Anomalous origin of RCA from left coronary sinus,
50 year old male - Case7:
A case of RCA CTO
by Dr. Chiung-Jen Wu and Dr. Swapnil Mate
Case7: A case of RCA CTO by Dr. Chiung-Jen Wu and Dr. Swapnil Mate
Case
A 85 years old gentleman with hypertension presented with unstable angina and underwent PCI to LAD with two overlapping DES.
Staged PCI was performed to RCA CTO.
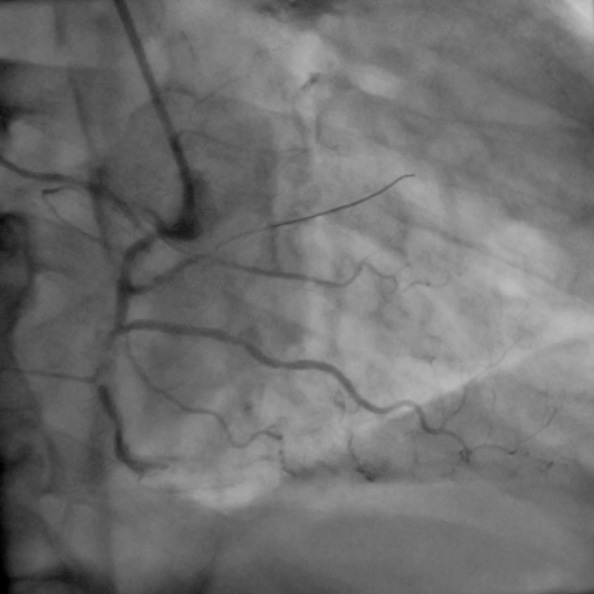
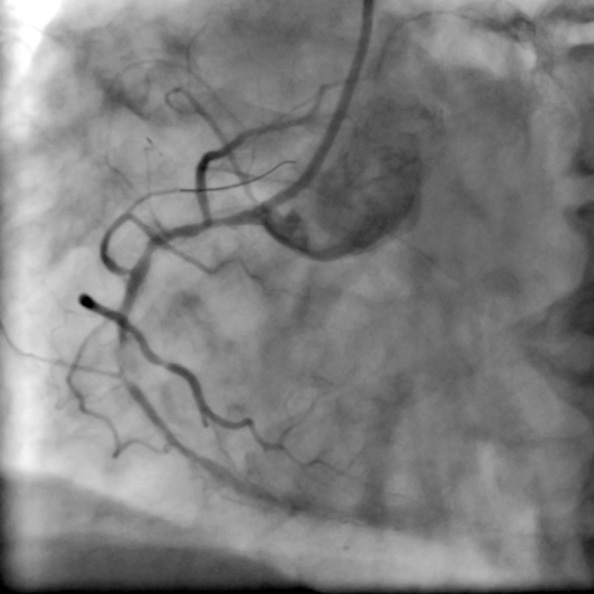
chronic total occlusion at the origin of RV branch with distal vessel filling via grade II collaterals from left system
Left radial artery access
IKARI LET 4.0 guiding catheter
With the same guide support,a Runthrough guidewire was advanced to RV branch. A XT-A guidewire in a 130 cm Finecross MC was attempted to cross the CTO, however the MC could not be delivered till mid RCA CTO. The stenotic lesion in proximal segment was dilated with a MINITREK 2 x 20 mm balloon at 20 atm. Now MC could be passed till mid RCA. Wire escalation was done till GAIA Second wire could cross the lesion. MC could not cross the lesion even with balloon anchor in RV branch. A MINITREK 1.2 x 12 mm could cross the lesion with after deep cannulation of IL 4.0 guiding catheter and balloon anchor in RV branch (FIGURE 3). The lesion was serially dilated with 2.0, 2.5 and 3.0mm balloons. With the help of 3.0 mm balloon support IL 4.0 was advanced into RCA for deep cannulation and good support. A DES XIENCE EXPEDITION 2.75 x 48 mm stent could be delivered due to these manuvers (FIGURE 4) which was deployed at 12 atm, followed by postdilation with ACCUFORCE 3.0 x 20 balloon. Compromised RV branch was rescued with a Runthrough wire and MINITREK 1.2 x 12 mm balloon followed by MINITREK 2.0 x 20 balloon and kissing balloon dilation(2.0 balloon in RV and 3.0 mm in RCA). TIMI 3 flow and 18 % stenosis was achieved (FIGURE 5 & 6).
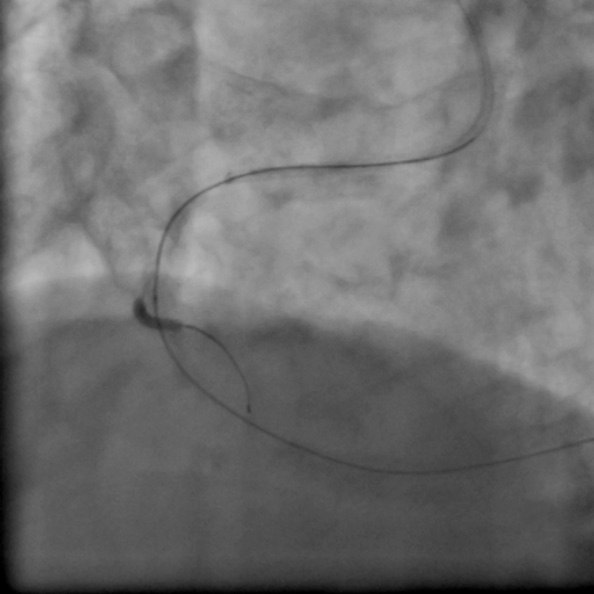
With the same guide support,a Runthrough guidewire was advanced to RV branch. A XT-A guidewire in a 130 cm Finecross MC was attempted to cross the CTO, however the MC could not be delivered till mid RCA CTO. The stenotic lesion in proximal segment was dilated with a MINITREK 2 x 20 mm balloon at 20 atm. Now MC could be passed till mid RCA. Wire escalation was done till GAIA Second wire could cross the lesion. MC could not cross the lesion even with balloon anchor in RV branch. A MINITREK 1.2 x 12 mm could cross the lesion with after deep cannulation of IL 4.0 guiding catheter and balloon anchor in RV branch.

The lesion was serially dilated with 2.0, 2.5 and 3.0mm balloons. With the help of 3.0 mm balloon support IL 4.0 was advanced into RCA for deep cannulation and good support. A DES XIENCE EXPEDITION 2.75 x 48 mm stent could be delivered due to these manuvers (FIGURE 4) which was deployed at 12 atm, followed by postdilation with ACCUFORCE 3.0 x 20 balloon.
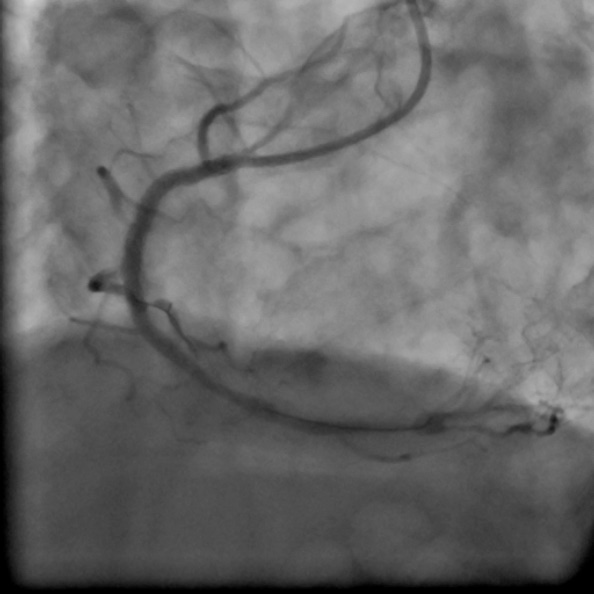

Compromised RV branch was rescued with a Runthrough wire and MINITREK 1.2 x 12 mm balloon followed by MINITREK 2.0 x 20 balloon and kissing balloon dilation(2.0 balloon in RV and 3.0 mm in RCA). TIMI 3 flow and 18 % stenosis was achieved.

Dr. Chiung-Jen Wu, Dr. Swapnil Mate and colleagues
- ← Prev
- Next →
